Thursday, January 4, 2018
Thursday, November 30, 2017
Majoring in Chronic Illness Management with a Minor in Applied Nursing
Seriously guys. Every time I hear those commercials for continuing education that say things like, "get credit for military experience!" or "use job skills to get an accelerated degree!" I think... man... if only they gave out degrees keeping yourself alive with chronic illnesses. I have a lot of spoonie friends and every single one of them should get to add C.P.P. (certified professional patient) to the end of their title in addition to an honorary nursing degree for many of them. For those of you who don't get a peak into this aspect of my life, here are some of the behind the scenes tasks needed to function.
Medication Management
This takes up SO. MUCH. FREAKIN. TIME. You have to make sure all your meds are cleared with all your specialists because they don't chat, you have to make sure no new meds will kill you (allergies, interactions, effect on other conditions), you have to get the script, send it to the pharmacy (assuming they have it), pick it up or set up shipment, keep track of refills, separately order all your OTC meds and supplements, sort out medication or check if medication is presorted correctly, make sure any ED staff, EMS, or doctor can access what prescriptions you are on at any point in time, fight insurance, pay bills, likely deal with 2-3 pharmacies, infusion companies, specialty pharmacies, mail order pharmacies, and actually remember to take them and have rescue meds with you at all times. But yeah... just that. Add secretary and applied pharmacist to your CV.
Appointment Scheduling, Cancellations, and Heckling
This one might be my LEAST favorite. Doctors and other medical professionals have a HUGE range in availability, responsiveness, attitudes towards collaboration and remote patient contact. I hate talking on the phone. I hate talking to people I don't know in general. People find it hard to understand me and I have a hard time understanding them. It isn't a great combo. But I do it because I have to. Generally, my team falls into two categories: can see you within the week or can see you in the next 3-9 months. While I totally get the deal with both types, it can be more than frustrating for something to come up in between your 3-9 month follow ups. I am currently playing phone tag and portal spamming with my GI teams because things need getting done but have been less than successful.
As mycharliequinn so aptly explains going to the doctor as a spoonie: "going to the doctor when you're chronically ill is weird. It's like imagine everything in your house is on fire, and you're standing there and the fire department come[s] in like, describe the fire to me and maybe we can find out what caused it and put it out. And you can't just say everything so you're like... well the fire in the curtain is the biggest but the fire in the photo albums might be doing the most damage also the fire in the couch is really inconvenient. Occasionally the fire guy is like, well your tv is on fire so it might be electronic- fireitus but that would cause other things like fire in the DVD player. And you're like, oh yes. That's been on fire for years. I forgot to mention it because it's always been a relatively small fire. It's right next to the bookshelf which has much more fire. And then the fire guy is like, oh. I wouldn't worry about that, book shelf fire just happens sometimes."

Attending your "Weekly" Appointments
For me, I am currently on a "rather empty" schedule with weekly PT and Aqua PT sessions and biweekly infusions. Just getting those scheduled and being able to get to them and participate takes a lot of spoons and most of my schedule is based off these events.
Decide When to Brave Emergency Departments
Practically have an algorithm this one now but can be tricky, especially considering the "luck of the draw" on if your ED team has even heard of your conditions, actually pays attention to your chart, or can do anything to help. Chronic illnesses often leave you in this limbo where you're not about to drop dead but not okay enough to stay home and NO WAY can get in to see your 3-9 month doc who manages that kind of stuff. It can be awkward for everyone.
Sunday, October 29, 2017
Tips for an Inclusive Halloween
Halloween can be a real struggle for kids (and adults) with disabilities. Here are some examples of aspects of halloween that are not accessible:


- Walking around in the dark
- Being surrounded by people who look different than normal
- Sensory considerations with costumes
- Sensory considerations with house decorations (flashing lights, motion activated stuff, jump scares)
- Lots of walking/ rolling and physical accessibility of getting to house's doors
- Talking to strangers (Trick or treat, asking for candy, responding to what your costume is)
- Food allergies or inability to eat
- Fine motor skills needed to grab candy
Here are a few adaptations/considerations that will help mitigate these challenges:
Food allergies/ inability to eat: Meet the Teal Pumpkin Project
The Teal Pumpkin Project is an initiative to include those with food allergies or special diets in trick-or-treating and to raise awareness. To participate paint a pumpkin teal (or print a picture and tape it to your door) and stick it on your porch. When you go out to buy candy, also buy some non-food items for kids. Examples: silly bands, party favors, bouncy balls, silly putty, vampire teeth or stickers! Party stores have lots of this stuff! Then, when trick or treaters come, simply hold two bowls and let the child choose! Believe it or not, there are even some kids who just don't like candy (real bummer for Halloween).
Resources and further details found here! This year they have even added a map where you can tell the world your house is participating!
Trick or Treaters who don't say Trick or Treat
There can be many reasons why someone might not verbal say trick or treat. They may be deaf, have anxiety related speech issues, be nonverbal, or just unaware that they are supposed to/why they are supposed to. Some may carry cards like this. Some may have a communication device. Some may just expect you give them candy. When in doubt, just give the kid some candy!
Decorating Your House
Keep in mind that for kids, terrifying is more likely to mean they will skip your house rather than bravely wandering forward. Be careful of extension cords as tripping hazards, poorly lit uneven surfaces, steps needed to climb to get candy ratio and other dangerous factors that might be hard to see at night, kids are unpredictable and hopped up on sugar. Also consider use of strobe lights, fog machines, and motion activated decorations as they may cause sensory overload, breathing issues, seizures etc. If you do want to use a strobe light, set it at a lower interval and it will be less likely to cause problems. Remember: its about the candy, costumes and fun...
Pro Tip: If you live in a house with more than 5 steps you might want to consider sitting down by the sidewalk during the main rush to hand out candy if you don't want to get skipped!
Be patient and Enjoy!
Give that kid who appear to be indecisive a little extra time to look at his options, he might have allergies, motor planning issues, or just wants to get candy he actually likes instead of accidentally grabbing the stinkin pretzel bag. Don't force children to speak to get candy. Give compliments on costumes even if you have no idea what they just said they were but also keep in mind that a kid not wearing a costume may have sensory issues, fabric allergies, or is scared of costumes. Also, if a teenager, adult, or other non-kid comes to you trick or treating don't make them feel out of place, they're participating and nothing wrong with being a kid at heart!

HAPPY HALLOWEEN!
Tuesday, October 10, 2017
Me vs Gravity: Life with Dysautonomia


October is also Dysautonomia Awareness Month! Wahoo! Dysautonomia is an umbrella term for several conditions that result from a dysfunction of the autonomic nervous system (ANS). Many people know of the ANS from health class as being the system that is in charge of the "fight or flight" response, and you'd be mostly right. Yes, the ANS is in charge of "fight or flight" but more broadly, it is essentially in charge of regulating the automatic functions of your body. There are nine different types of dysautonomia: POTS, OI, AAG, Pandys, NMH, NCS, PAF, FD, and MSA. Learn more about them here. For this post I will only be talking about POTS and my experiences with POTS. I have secondary hyperadenergic POTS (hPOTS).
 What is POTS?
What is POTS?

{kind=link}
As stated above, POTS is a neurological condition in which the ANS does not send the proper signals to the body to regulate blood pressure and heart rate (primarily, POTS affects the whole body). Normally, when a person stands, gravity pulls blood to the lower extremities. The nervous system senses this and sends a message to the blood vessels to constrict, sending more blood back to the heart and head. With POTS, this message to constrict does not get sent. Therefore, instead of the heart rate increasing by a normal 10 to 15 bpm upon standing, it can increase by more than 30 and can even double (when first diagnosed mine went from 68 bpm lying down to 189 bpm and remained that way for 10+ minutes). By affecting circulation, it also affects cerebral blood flow. Symptoms include orthostatic intolerance (dizziness), chest pain, headaches, GI cramps and dysmotility, inability to focus and concentrate for long periods of time, inability to read due to blurred vision, difficulty with recall, blood pooling, extreme fatigue, nausea, tremulousness, insomnia, loss of consciousness.
What causes POTS?
While there is some knowledge about comorbid conditions that are commonly seen with POTS and certain types of POTS have associated causes with the start of symptoms, it is unknown what is the true cause. For example, one type of POTS can occur post-concussion and we know that but not everyone who gets a concussion gets POTS. There is currently no cure and treatment is based on symptom management.
Common Misconceptions
- POTS is caused by anxiety. POTS symptoms can mimic anxiety/panic disorders patients are often misdiagnosed or POTS is missed entirely because symptoms are deemed to be caused by anxiety. See research here.
- POTS is caused by deconditioning. See research here. Exercise (for those allowed by their doctors) can be a crucial part of a POTS patient's treatment plan but is not caused by deconditioning and cannot be cured by exercise alone.
- POTS is just getting dizzy sometimes. POTS is a complex neurological condition that effects every patient different though almost all, if not all, have multiple organ systems effected.

Lingo
- brain fog: cloudy feeling that hangs around and causes you to do stupid shit like flush the toilet three times, forget if you took your meds or just thought about taking your meds, and being unable to form a coherent sentence
What my POTS is like
***Disclaimer: This will by no means be an extensive list of symptoms or experiences and this is just how POTS effects me. There will also be crossover between EDS, GP, MCAD and possibly LQTS.***
I was formally diagnosed with POTS in 2015 though I had symptoms beginning in early middle school years. To save my fingers I am just going to talk about my current life with POTS and will probably do a more extensive post later, I just tired and lazy.
Remember the last time you had the flu and ached everywhere, slept all day and don't remember half of what happened? Now imagine waking up feeling like that every day (and more! yaaay), this is one of my main struggles with POTS. Several factors contribute the fatigue including medication and adrenaline surges/crashes but on any given day my energy level is equal to or less than a sloth on Ambien. I take naps nearly daily, sometimes multiple times a day just to keep up with my peers. I have trouble filtering out stimuli, recalling things, producing speech, following multistep directions, and reading for comprehension.
 Another big problem I have is blood pooling. POTS alone can cause bad pooling but with the stretchiness of my veins from EDS, it is much worse. I also have Raynaud's syndrome so my hands and feet are always cold! The picture to the left is an example of blood pooling in my hands (on medication). This is what happens if I stand with one hand raised and one arm relaxed for two minutes. The white hand was raised and therefore has less pooling (gravity does all the work). After about a minute of sitting my legs look like my left hand. Now imagine a 11 hour car ride or a 3 hour lecture. This is why many POTSies wear compression stockings and socks to help our bodies circulate blood or why lying down with our legs up helps.
Another big problem I have is blood pooling. POTS alone can cause bad pooling but with the stretchiness of my veins from EDS, it is much worse. I also have Raynaud's syndrome so my hands and feet are always cold! The picture to the left is an example of blood pooling in my hands (on medication). This is what happens if I stand with one hand raised and one arm relaxed for two minutes. The white hand was raised and therefore has less pooling (gravity does all the work). After about a minute of sitting my legs look like my left hand. Now imagine a 11 hour car ride or a 3 hour lecture. This is why many POTSies wear compression stockings and socks to help our bodies circulate blood or why lying down with our legs up helps. 
While POTS impacts many things in my life it does not mean I can't do fun stuff, learn, and enjoy life I just need everything to slow down and take breaks. I have very limited energy and most is spent on school, existing, medical appointments, personal hygiene (showers are EXHAUSTING), and keeping myself alive. I have to worry about getting places without steps, lying down in the middle of the mall to keep myself from passing out, obsessing over hydration and medication schedules to maintain baseline and prevent things from spiraling out of control, and pretend to be a functioning adult.
Thanks for reading and make noise for turquoise (dysautonomia awareness color)!
Sunday, October 1, 2017
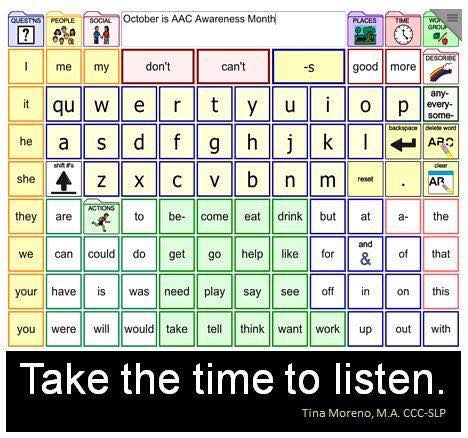
Not being able to speak is not the same as not having anything to say! AAC Awareness Month
Augmentative and Alternative Communication (AAC) is any form of communication that supplements or replaces speech. AAC can take many forms, from sign language to facial expressions, to printed communication books to high tech speech generating devices (SGDs AKA "talkers"). Basically, if it isn't speech it is AAC! High tech does not always mean better and just like study habits and treatment plans, what works for one person might not work well for another, even with the same diagnosis. AAC users are of all ages, genders, races, disabilities, and literacy levels but they all have either no speech, speech that is difficult to understand, or have trouble forming fluent speech.
Remember that last time you lost your voice? I can almost guarantee you that you became frustrated at least once during that time period. Now imagine that you have an itch on the center of your back and you cannot speak. You're only given this sheet of laminate paper.

You can't sign, speak, or write. How do you tell me your back itches? Maybe ... "I/me/me -- help -- turn..." then directional words until your communication partner happens upon the place your back itches??
Sounds "no want"? What? Not the word you were thinking of? Oh well... good enough. NO NO NO!

Above: An example of a SGD and computer controlled with the users eyes. For more information click here.
For a great website for AAC resources (use, teaching, awareness) click here (PrAACtical AAC)!

Remember that last time you lost your voice? I can almost guarantee you that you became frustrated at least once during that time period. Now imagine that you have an itch on the center of your back and you cannot speak. You're only given this sheet of laminate paper.

You can't sign, speak, or write. How do you tell me your back itches? Maybe ... "I/me/me -- help -- turn..." then directional words until your communication partner happens upon the place your back itches??
Sounds "no want"? What? Not the word you were thinking of? Oh well... good enough. NO NO NO!

Everybody should be given access to words (and symbols). Words are powerful and they make us who we are and allow us to connect with others. They surround us from the moment we are born to our very last breaths. Words are more than just basic needs and wants. Words are social, personal, creative and powerful. Nobody should have that kept from them.
Tips for Communicating with a person who uses AAC:
- Be patient! One of the most frustrating things for me if being asked a question and halfway through your response they say something like, "oh, nevermind" or "don't worry about it". Similarly, group conversations can be VERY difficult when it takes you longer to respond. I often form my answer and by time I have finished my response is irrelevant. Don't be offended if I tend to be quieter in groups, I am listening! I know it is hard to take the time to slow it down but I guaranteed you the AAC user will be very grateful!
- Don't limit to yes and no questions. It gets boring really quick. That being said, if an answer is needed quickly, it might be helpful to ask yes or no questions or give a few options to chose from. Ex. "Julie, the house is burning and I need to know, should we use: unicorn power, ninjas or rocks to stop the fire. Unicorn power? (yes/no) Ninjas? (yes/no) Rocks? (yes/no) Something else? (wait for response using AAC).
- Presume competence. Talk to us at an age appropriate level and normal volume and rate (unless known to have hearing or processing issues). POP QUIZ! (all based on actual experiences)
- Billy is 40 years old Giants fan and uses a speech generating device. When talking to Billy you should:
- HELLO BILLY BOY! HOW------------ARE---------YOU?!
- Hi Billy, how are you? I saw the Giants won last night!
- *turns to Billy's wife* Hi Betty! How are you? How is Billy doing?
- HI. My-------name--------is---------S-U-S-A-N. NIIIIIICCEEEE TO MEEET YOU! YOUR CHAIR IS SOOOOOO CUTE!
- If you answered #2, wahoo! You get it.
- Advocate with us and for us!
Cool AAC Related Stuff:
Above: Video compilation project showing AAC users doing various activities and living their lives!
For a great website for AAC resources (use, teaching, awareness) click here (PrAACtical AAC)!
Examples of popular low and high tech systems:
- Tobii Dynavox Products
- Pragmatic Organization Dynamic Display (AKA PODD) (PODD is available in light tech (books) and high tech (SGD formatted for Tobii devices or iPad)
- Prentke Romich (makers of LAMP Words for Life and UNITY software)
- Saltillo (NovaChat, TouchChat)
Getting Hip with the Lingo
- Augmentative and Alternative Communication (AAC): includes all forms of communication (other than oral speech) that are used to express thoughts, needs, wants, and ideas. We all use AAC when we make facial expressions or gestures, use symbols or pictures, or write (Source: ASHA)
- Speech-Generating Device: Any piece of technology that turns user inputted text or symbols and turns it into spoken computer generated or synthesized voice. AKA a machine that talks for you.
- Switch Access: using a switch to control your AAC device (like an automatic door switch). Switches can be activated using touch, light, sound, breath, or even tongue movements!
Tuesday, August 15, 2017
Sick of Silent Suffering
Over the past couple years I have become increasingly open about talking, writing, blogging, and advocating about things that are important to me, including my chronic illnesses but I definitely wasn’t always this way and my family, for all their wonderful other qualities, is more the suffer in silence type. That is how I grew up and it wasn’t until recently I realized the toll it has taken on me. *Side note: I do believe that this system works for some people and keep them happier, I’m not judging.* Back to glorious me. The problem with suffer in silence is that, intentionally or subconsciously, it creates a wall between you and “everyone else”. After all, how could you possibly know that another person was facing similar challenges as you if they are also silent? One of my most valued friendships is with someone that I despised in high school because she was getting help for what turned out to be the same condition I had (she hated me back because I flew under the radar). We reconnected after my diagnosis and confessed our mutual hatred for each other and turns out we are very similar people with similar struggles and challenges and we keep each other sane (lol, if you can call it that L.B.N). Yes, that is a extreme example but hang in there.
 We are social creatures. We strive to make connections with others, find the people who make us laugh and support us, and teach us about the world. We long to fit in, to be noticed, or even to be famous. But who here can say that they have felt it is easier or better or more desired to suffer in silence no matter how big or small the challenge is? I struggled through my education beating myself up along the way for not being able to figure out long division, for NEVER being able to spell things right, for trying to fit in harder than I tried to learn. Growing up in an area that prides academic achievement as a critical pillar of your existence, I felt like a failure even though I “made good grades and had good friends”. It wasn’t just academically either, family stress... silence, friend drama... silence, depression... silence, and pain... silence. Then I graduated and moved to Birmingham, AL. Which made it so. much. worse. There saving face is critical to social acceptance. It was suffocating for me and I’m fairly certain contributed to my physical and mental health getting so much worse. There is a great Miranda Lambert song (oh no Julie... not country. Yes. Country.) called “Mama’s Broken Heart” about a breakup and saving face. It “don’t matter how you feel, it only matters how you look... my mama came from a softer generation where you get a grip and bite your lip just to save a little face”.
We are social creatures. We strive to make connections with others, find the people who make us laugh and support us, and teach us about the world. We long to fit in, to be noticed, or even to be famous. But who here can say that they have felt it is easier or better or more desired to suffer in silence no matter how big or small the challenge is? I struggled through my education beating myself up along the way for not being able to figure out long division, for NEVER being able to spell things right, for trying to fit in harder than I tried to learn. Growing up in an area that prides academic achievement as a critical pillar of your existence, I felt like a failure even though I “made good grades and had good friends”. It wasn’t just academically either, family stress... silence, friend drama... silence, depression... silence, and pain... silence. Then I graduated and moved to Birmingham, AL. Which made it so. much. worse. There saving face is critical to social acceptance. It was suffocating for me and I’m fairly certain contributed to my physical and mental health getting so much worse. There is a great Miranda Lambert song (oh no Julie... not country. Yes. Country.) called “Mama’s Broken Heart” about a breakup and saving face. It “don’t matter how you feel, it only matters how you look... my mama came from a softer generation where you get a grip and bite your lip just to save a little face”.
So I left and moved back here and that is when I decided to stop hiding and start being open about all kinds of things and I have been amazed at where it has lead me. I have accepted the vulnerability that comes with exposing hurt, weakness, and challenges and through it have gained truly amazing friends, education, healing and perspective. I no longer feel totally alone in this world which I am remind of even in my worst days by the true connections I have made with others. I am learning to express myself, care for myself, and help others. I truly believe that vulnerability leads to connection and connection leads to understanding and understanding leads to compassion and compassion... well compassion is pretty powerful stuff.
“The irony that we attempt to disown our difficult stories to appear more whole or more acceptable but our wholeness - even our wholeheartedness- actually depends on the integration of all our experiences including the falls. “ -Brene Brown
Wednesday, August 9, 2017
Life Hacks: Spoonie College Edition
So I'm actually starting my 5th year of college going straight (fall, spring and summer except one summer). I have attended three different universities and started out only minimally effected by health problems (mostly GI, migraines) and wound up here, a professional patient needing complex care and supports. While each college had different systems, strengths and difficulties, I learned some valuable things about being successful in an environment that is largely unsuited for those with chronic illnesses.
Here are some things I have learned along the way, in no particular order and not institution specific:
- Disability services: The process towards getting accommodations is LONG, often repetitive, and stressful. Often, accommodations are generic, inflexible, and "base packaged" (you probably will get about (max) half the things you need to keep up and be successful and the rest is up to you. Here are some tips to get the most out of the services offered there (and your time and energy):
- Start paperwork ASAP, pester those overworked doctors to get their part in before the semester starts as accommodations will never be retroactive. Also, make copies/ scans of every form or piece of documentation that leaves your hands. Things get lost all the time.
- Know which battles to fight. Back to the max 50% of what you need thing, often times you will receive basic accommodation and get some pushback asking for more. Is that note taker necessary for you to succeed or can you work out a way to record lectures, ask a classmate to look at theirs, use assistive technology and save your fight for extended time on tests where you might fail without it.
- Send a personal note/make a personal introduction along with your formal accommodations sheet. In my experience, this has helped teachers relate to me, understand how my disabilities effect me and my learning/schooling, and also makes it seem a lot less like taking passes on things and more like "I expect this to happen, I don't know when or where or how, but here's a proactive heads up". It isn't necessary to name or intricately discuss your diagnoses to be effective.
- You'll have to do a lot of accommodating for yourself/ working 1:1 with teachers.
- In most universities, students with disabilities have priority class registration. SUPER HELPFUL!!!
- Housing: While living on campus may at first seem unappealing (again, varies in atmosphere by university), there can be a lot of benefits especially if you can't drive.
- They are required to have ADA accessible rooms. My room has widened doors, a lower peephole, lower closet bars, grab bars in the bathroom and shower, a fold down shower bench, and lowered light switches.
- Accommodations for single rooms can be made for those with compromised immune systems, PCAs, MCAD, severe GI issues, and other medical reasons.
- You can have a quiet place to rest in between classes, are close to dining (if you eat), and have access to evening events such as clubs, performances, and hanging out with friends without being too far from home or living in the Student Union Building.
- DOWNSIDE #1: If you have problems that can be exacerbated by fire alarms... apparently no one knows how to cook MFing popcorn.
- DOWNSIDE #2: Germs spread fast and easy, may not be the safest place if you have a weak immune system without taking precautions.
- Class Schedule Advice
- What you want isn't always what is best. Sure, like nobody wants 9 AMs every day... or any day... but for me, the later in the day the more medication wears off, pain increases, spasticity increases, and overall deterioration occurs. Class is already hard enough to sit through, concentrate, learn and remember... don't make it harder on yourself for a potential 2-3 more hours of sleep. Or flip all that if that's how your body works.
- Register ASAP. Classes fill up, plans change.
- Schedule max number possible classes, attend all the first week and then drop as needed. That way you secure your seat, get to meet the professor, see the syllabus, see if there are major barriers in the class (i.e. Service dog you're allergic to in a small classroom)
- Medical care/ health safety
- If you live on campus, tape a folder somewhere visible (wall, by light, dresser) and write EMERGENCY INFO on it super big and put in your medical emergency info, copy of your license/state ID card, insurance card (if you have it), and your school ID/student ID #
- Start a file with on campus health. Even if they never care for you it is helpful for them to have your base information in case you need them in an urgent matter, have doctors far away, or just need something simple like a wound cleaned. Most student health offices will be able to do allergy shots, some will even help manage infusions.
- Introduce yourself to the campus chief of police, especially if you have the potential for reoccurring EMS issues like seizures, anaphylaxis, diabetes etc. They are usually first on the scene and can inform EMS.
- Wear a medical ID bracelet. Bonus if it has a way to see all your info. See my post on my system here.
- If you have asthma, MCAD, or immune problems I highly suggest purchasing a high quality, relatively comfortable mask to wear outside around campus. I pass smokers, high perfumers, and other triggers CONSTANTLY on campus. I use these and love them (recommend the ones with 2 filters for comfort and breathability).

- Miscellaneous
- Join one club. Even if you only go twice a year, you may meet some people and you feel somewhat a part of things.
- If you live on campus, get to know some people on your floor. They may be good for procrastination buddies, errand helpers, cards against humanity mates, or near family friends.
- Don't bring everything you own to move-in. Stuff accumulates anyways and it is a pain.

Hope this helps. It can be overwhelming but it IS manageable with the right supports.

Subscribe to:
Posts (Atom)